Arthritis and Shoulder Joint Replacement
There are two main causes of arthritis of the shoulder: ‘Wear & Tear' osteoarthritis and rheumatoid arthritis
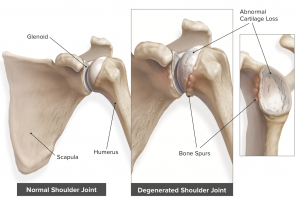
Osteoarthritis of the shoulder is actually quite uncommon. It is nothing like as common as arthritis of the knee or hip. It is probably a disorder with a strong genetic influence. The bearing surface is slowly destroyed, so that ultimately bone is grating on bone, like a wheel with a tyre. Extra bone ‘spurs’, grow round the edge, blocking movement.
Treatment:
There are four different treatments for arthritis of the shoulder:
- Medications – analgesics and anti-inflammatory tablets
- Physiotherapy
- Cortisone injections
- Joint Replacement surgery
Most patients will usually have exhausted medications by the time they seek specialist help. Physiotherapy is often useful and should be attempted before contemplating surgery. Cortisone injections can be of huge benefit in patients with arthritis. They can give rise to pain relief for many months. Unfortunately their effect wanes each time they are repeated. They do not damage the joint and they do not affect the patient generally.
Surgery is only considered when everything else has failed to restore the patient's quality of life to a reasonable level. Though keyhole surgery is available, it seldom gives rise to sufficient benefit. Joint replacement surgery has been available for at least thirty years and modern techniques have a very high success and satisfaction rate. As with other joint replacements, the bearing is resurfaced with metal and plastic and this gives rise to terrific pain relief and restoration of function.
Surgery:
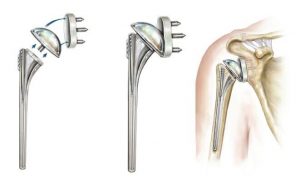
Shoulder Joint replacement involves removing the ball and socket and replacing it with a metal ball and a plastic socket. There can be no pain felt from the new joint, so pain is eradicated.
What the patient has to go through The patient is admitted on the day of surgery. The operation is usually performed under general anaesthetic with a nerve block, which prevents pain immediately after the surgery. It can be performed without a general anaesthetic. The surgery takes around ninety minutes.
An incision is made down the front of the shoulder. The patient wakes with his arm in a sling and no feeling in it because of the nerve block. This lasts around twelve hours, then the sensation and movement returns. Pain killers are administered.
The day after the surgery, the patient can get out of bed and walk around with the arm in the sling. Patients may go in the shower and may get the wound wet. They may get dressed in normal clothes but will still need the sling. The shoulder is acutely painful for two weeks and moderately painful for six weeks. Patients may discard the sling after three weeks, but most will wear it on and off for the full six weeks.
Physiotherapy and exercises are commenced immediately after the surgery and continue for at least three months. Patients cannot drive for at least six and often eight weeks. Patients do not notice much benefit from the surgery for six weeks, but after three months the pain relief is usually dramatic. It takes at least four months for the stiffness to resolve. The shoulder continues to improve for a year.
Results:
This surgery has in excess of a 90% success rate in terms of pain relief. In patients with osteoarthritis, there will usually be an increased range of movement.
What can go wrong?
The biggest initial problem is infection. This is rare, less than 2%. If it occurs, it can be dealt with, but repeated surgery and a poor result may ensue . There are other rare problems including nerve damage, bone breakage and dislocation.
How long does the operation/joint replacement last?
In simple terms, around twenty years. You need to discuss this with your surgeon.
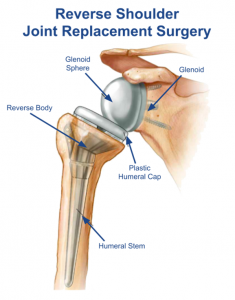
Rotator Cuff Arthritis
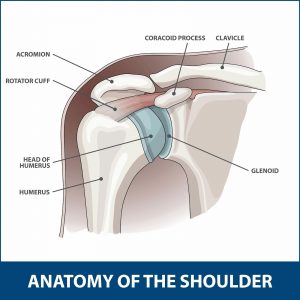
The commonest form of arthritis type problems with the shoulder can be called Rotator Cuff Arthritis. The rotator cuff is a muscle which powers the shoulder and in some people, as they age, the tendons fray and break, like an old rope! That muscle no longer works and the patient cannot lift their arm. Like a frayed rope, it can’t be repaired, so another solution is necessary.
The solution is completely bizarre. It turns out that one can manage with that part of the rotator cuff, if a special replacement is performed. For this, the ball of the shoulder is converted to a socket and the socket to a ball, so a so-called Reverse Shoulder Replacement. Sometimes there is also arthritis but often there is not. So this is just done as a sort of muscle improving operation. Patients are able to reach up above their heads but one limitation is reduced ability to reach round behind the back, above the belt.